
Oncology
Oncology
Overview
We are a clinical stage biopharmaceutical company focused on the discovery and development of covalent small molecules to treat patients with genetically defined cancers and metabolic diseases. A covalent small molecule is a synthetic compound that forms a permanent bond to its target protein and offers a number of potential advantages over conventional non-covalent drugs, including greater target selectivity, lower drug exposure, and the ability to drive a deeper, more durable response.
We are utilizing our proprietary FUSION™ System to discover, design and develop a pipeline of next-generation covalent-binding small molecule medicines designed to maximize clinical benefit for patients with various cancers and metabolic diseases, including diabetes. We aim to cure.
The following table summarizes our product candidate pipeline. We own full worldwide development and commercialization rights to all of our programs.
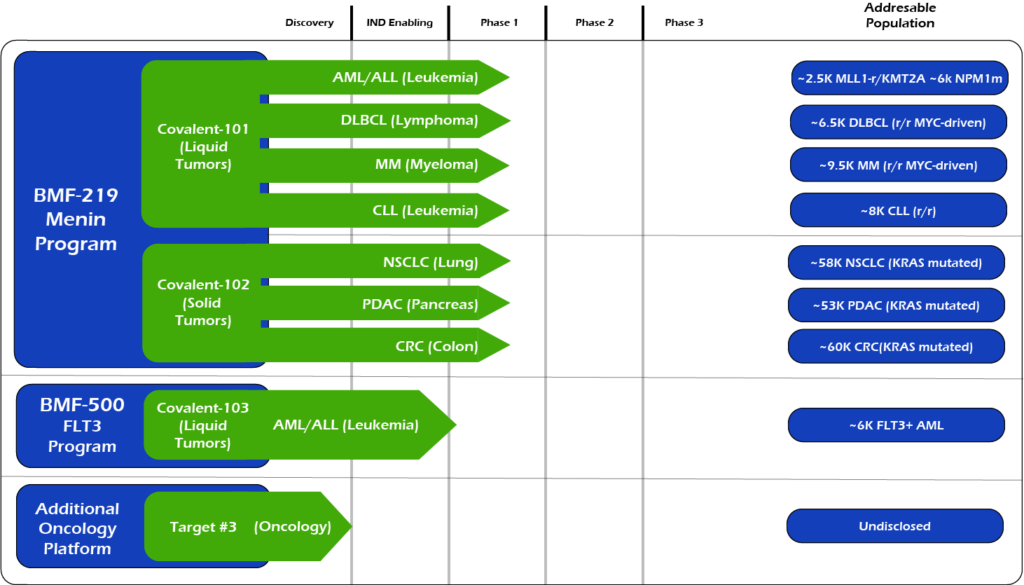
All our assets are in house designed, developed, and wholly owned by Biomea Fusion Inc.
BMF-219 – Menin Inhibitor in Oncology
BMF-219 is a covalently binding inhibitor of menin, a protein known to play an essential role in oncogenic signaling in genetically defined leukemias as well as in diabetes. Preclinically, BMF-219 has demonstrated in well-established acute leukemia cell lines robust downregulation of key leukemogenic genes in addition to menin itself. Additionally, BMF-219 has shown anticancer activity in multiple in vitro, in vivo, and ex vivo models of acute leukemia, multiple myeloma, diffuse large B-cell lymphoma and chronic lymphocytic leukemia.
BMF-219 is currently being evaluated in first-in-human clinical trials enrolling patients with specific menin-dependent mutations in liquid and solid tumors as well as patients with diabetes.
MLLr/mNPM1 Dependent AML/ALL
Approximately 20,000 and 6,000 patients in the United States are diagnosed annually with AML and ALL, respectively. MLL-r leukemia has limited therapeutic options and affects approximately 10% of acute leukemias in adults and approximately 70% of acute leukemias in infants. In addition to MLL-r, MLL signaling in some forms of MLL wild-type (MLL-wt) AML have also been implicated, including those bearing independent oncogenic mutations in nucleophosmin (NPM1), a molecular chaperone, and DNA-methyltransferase 3A (DNMT3A), a methyl transferase. These subpopulations together represent approximately 45% of AML cases.
Patients with MLL rearrangements often suffer from failure of induction therapy or disease relapse, resulting in poor clinical outcomes. In pediatric AML, the
five-year event-free survival rate on average is 44% but ranges between 11% and 92% depending on the MLL-translocation subtypes. In ALL, the five-year survival rate for people aged 20 and older is approximately 37% and for people under the age of 20 it is approximately 89%. However, pediatric MLL-r ALL patients fare much worse, with four-year survival rates as low as 10%, compared to 64% for those without MLL rearrangements.
A perhaps more dire area of unmet need is relapsed/refractory AML. Despite evolving insights into the pathogenesis of AML, over 11,000 patients with AML die each year from the disease in the United States. Relapse is the most common cause of treatment failure. The five-year overall survival (OS) for adult patients with AML after disease relapse is only approximately 10%. Furthermore, a published study showed that approximately 20% of patients demonstrated primary induction failure adding even more patients to this refractory category. Currently, allogeneic hematopoietic cell transplantation (HCT) is considered to be the only reliable option with curative potential, with OS estimated between 15% to 25% three to five years post-transplant. To improve overall quality of life for patients, physicians are favoring oral targeted agents and strategies that avoid intensive chemotherapy and prolonged inpatient admissions. Key in this effort is a focus on molecular testing to identify the potential for targeted therapies.
Given the involvement of MLL and NPM1 in a high percentage of acute leukemias, and the poor clinical outcomes provided by available treatments, we believe a new treatment that can inhibit the function of both targets by disrupting or preventing interactions with menin could address this unmet need.
Clinical Development
In July 2023, Biomea reported initial topline data showcasing initial responses in r/r AML patients with menin-dependent mutations. BMF-219 was generally well tolerated with no dose-limiting toxicities observed, and no QTc prolongation reported.
In December 2023, the achievement of MRD-neg in first complete responder with AML was reported.
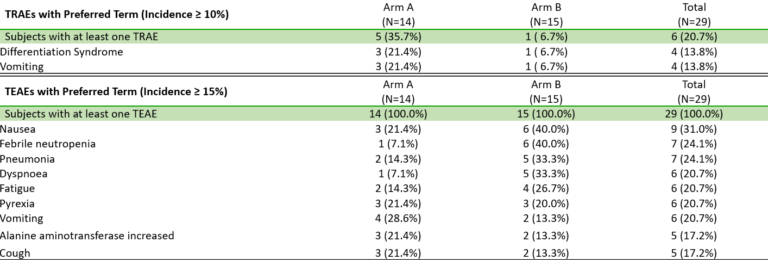
Fig. BMF-219 is Well Tolerated, Allowing for Continued Dose Escalation (Lancet et al. ASH 2023)
MYC Driven Liquid Tumors (MM, DLBCL, CLL)
Non-Small Cell Lung Cancer is the most common form of lung cancer, representing ~84% of all lung cancer cases or approximately 200,000 cases in the U.S. each year (Source: NCI SEER Data). Additionally, the five-year survival rate of NSCLC is ~25%. While lung cancer is the 3rd most common form of cancer in the U.S. based on incidence, lung cancer contributes to the highest number of annual cancer deaths in the U.S. KRAS is a key node in the RAS signaling pathway, which can be oncogenic. KRAS is the most frequent oncogene in NSCLC, occurring in ~30% of patients with NSCLC. Notably, RAS signaling is known to result in active MYC, which can facilitate pro-tumor transcriptional processes. KRAS inhibitors have shown efficacy in KRAS mutant NSCLC patients in clinical trials.
Pancreatic cancer is a relatively rare form of cancer in the U.S., representing approximately 60,000 cases in the U.S. each year (Source: NCI SEER Data). Pancreatic cancer is an aggressive cancer with a very low five-year survival rate of ~11%, indicating that there is a large unmet need. It is rarely diagnosed early, contributing to the low survival rate. Among patients with pancreatic cancer, RAS mutations (including KRAS) occur in up to approximately 98% of patients.
Colorectal cancer is the fourth most common form of cancer in the U.S., representing approximately 150,000 cases in the U.S. each year (Source: NCI SEER Data). These cancers start in the rectum or the colon and can be diagnosed/identified early, even potentially as noncancerous polyps. The five-year survival rate of CRC is approximately 65%. Among other mutations, KRAS mutations occur in approximately 50% of patients with CRC.
BMF-500 - FLT3 Inhibitor in AML
BMF-500 is an investigational, novel, orally bioavailable, highly potent and selective covalent small molecule inhibitor of fms-like tyrosine kinase 3 (FLT3). Biomea has continued advancing BMF-500 toward the clinic, with investigational new drug (IND) application cleared in 1H2023 and initiated a Phase I study of BMF-500 (COVALENT-103; NCT05918692).
BMF-500 was discovered and developed in-house at Biomea using the company’s proprietary FUSION™ System and has demonstrated best-of-class potential based on extensive preclinical studies. The kinase profile of BMF-500 showed high target selectivity, suggesting the potential for minimal off-target liabilities. BMF-500 was designed to have a therapeutic profile to allow for combinations with standard of care and/or novel targeted agents like BMF-219.
FLT3 is a receptor tyrosine kinase (RTK) that plays a central role in the survival, proliferation, and differentiation of immature blood cells. Notably, FLT3 gene mutations are common in patients with AML and are associated with a poor prognosis. Nearly 30% of AML patients have a FLT3 mutation, representing more than 6,000 incident patients in the United States each year. While FLT3-specific and pan-tyrosine kinase inhibitors are approved by the FDA across various lines of therapy in AML, these agents have produced relatively low rates of durable responses and overall survival remains an unmet need.
Previous data presented at medical conferences showed BMF-500’s picomolar affinity to activating FLT3 mutations, including FLT3-ITD and various tyrosine kinase domain (TKD) mutations (Law et al. ASH 2022). BMF-500 demonstrated multi-fold higher potency and increased cytotoxicity than commercially available non-covalent FLT3 inhibitor gilteritinib. Further data also exhibited the potential utility of combination strategies to achieve higher antileukemic cell killing with reduced concentrations of BMF-500 and BMF-219 (Law et al. AACR 2023). These data provide preclinical evidence for combining pathway-specific inhibitors as a promising therapeutic strategy for further investigation in acute leukemia.
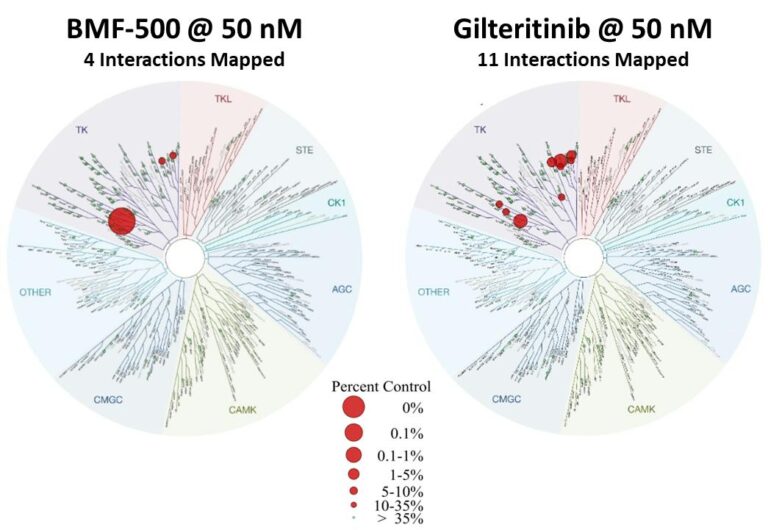
Fig. BMF-500 is highly selective to FLT3 (Law et al. ASH 2022).
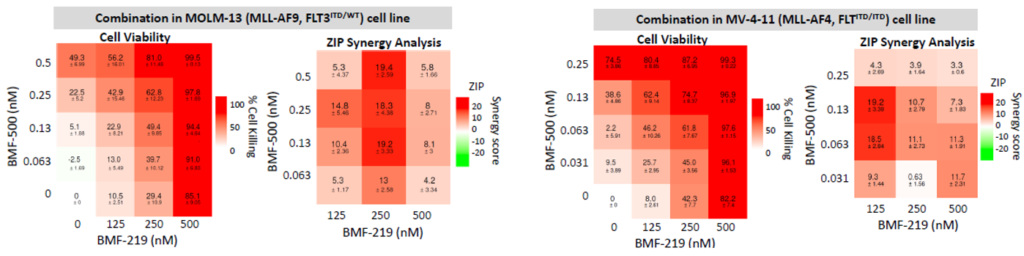
Fig. BMF-219 and BMF-500 in Combination Induced Higher Cell Killing at Lower Single Agent Concentrations (Law et al., AACR 2023)